Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay
Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay
Nasogastric (NG) tubes are mainly used for feeding, deflation, and drainage. The placement of NG tubes in infants is a common practice undertaken by nurses and increasingly by cares. It is often the responsibility of the pediatric nurse to ensure that an NG tube is properly sited. The prevalence of tube errors is not easy to ascertain because of the differing descriptions across the reported studies. However, Ellett and Beckstrand (1999) reported tube error rates in infants as high as 43.5 percent.
Verifying the placement of an NG tube is not only vital on insertion but also on subsequent use. Coughing, sneezing, and vomiting are all common causes of tube displacement in infants (Guenter and Silkroski 2001).Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay. NG tubes can easily be displaced on placing or after placement has been confirmed and often with no accompanying clinical signs (Metheny et al 1986). Even though displaced NG tubes carry associated morbidity and mortality, many nurses continue to be uninformed of the potential risks associated with their insertion and subsequent management (Cannaby et al 2002).
If insertion of the NG tube cannot be confirmed it should be removed and repositioned. There can be a reluctance to replace an NG tube because of the known distress caused to infants, staff (Holden et al 1997). Additional time and resources are essential for the necessary psychological preparation of the child. In addition, any vagueness in tube placement may lead to inadvertent removal of a correctly positioned tube, with unpleasant consequences for the infant.
In the event that prompted this review, two experienced nurses had followed recommended practice but a nasogastric tube was displaced in a conscious young person, resulting in pneumonitis. When not capable to obtain aspirate, the nurses used auscultation and confirmed the presence of a whoosh of air. They proceeded to use the nasogastric tube to administer drugs and the child remained asymptomatic during and for a substantial period following the course of action.
ORDER A PLAGIARISM-FREE PAPER NOW
A nasogastric (NG) tube is a small tube that goes into the stomach through the nose. Breast milk, formula, or liquid food is given through the tube directly into the stomach, giving your child extra calories. Feeding this way helps your child get enough nutrition to grow, develop, recover from illness, play, and learn. Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay.
Tube feeding can be done for children of any age. Some children will depend on tube feeding only until they are able to eat by mouth. Using the gastrointestinal (GI) tract for feedings keeps it healthy and working normally.
Other children can continue to eat as usual, and also get tube feedings for extra calories.
There are several ways to give an NG feeding. The type of tube, how often it needs to be changed, type and amount of formula, and length of feeding time will be decided by the doctor and dietitian, depending on your child’s needs.
Follow only the checked instructions in this sheet.
Your child’s special instructions:Type and size of feeding tube: ___ Change the feeding tube every: ___ Do not change the feeding tube yourself. What to feed: Amount to feed: How often to feed: Method: ___ bolus ___ continuous Type of pump: Rate of feeding: Flush the feeding tube at the end of each feeding with ml of warm water. Other: Measurement: Care of feeding bag and tubing:___ Change every day. If the bag and tubing do not clean easily, try using a solution made of equal amounts of white vinegar and cool water (for example 1 cup vinegar with 1 cup water). Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay. Rinse well and store in refrigerator. Throw away the feeding bag and tubing after 1 week; sooner if you cannot get it clean or if it begins to leak. |
Definitions
| aspiration | getting fluid into the lungs, which can cause trouble breathing |
| bolus | feeding over a short time |
| continuous | feeding over an extended time |
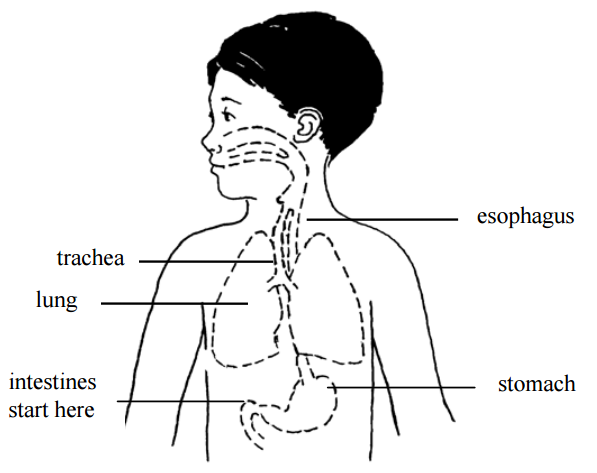
| GI tract | the esophagus, stomach, and intestines |
| gavage tube | another name for feeding tube; may be put in through mouth |
| lubricant | water-soluble substance such as K-Y® jelly, used to help the tube slip in more easily – do not use Vaseline® |
___ Inserting the feeding tube
It takes time and practice to learn how to insert the tube, so be patient with yourself. Do this by yourself only after you have done it successfully with the nurse present.
Get ready:
- Wash your hands.
- Gather supplies:
- feeding tube
- tape measure
- With your fingers, find your child’s sternum (breastbone). Gently feel the bone in the center of the chest, and then find its bottom edge. It will be below nipple level, and you will feel the bottom of the rib cage curving away to each side.
- Now imagine a spot on your child’s belly that is midway between the belly button and the bottom edge of the breastbone.Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay. Keep that spot in mind.
- Using a tape measure, measure from the tip of your child’s nose to the bottom of the earlobe, then down to that spot midway between belly button and breastbone edge. Write that number down: we will call it “your child’s measurement.” Measurement:
In this picture, the child’s measurement is 12 inches (3 inches from nose to ear, plus another 9 inches down).
- Now measure the tube (or find its length on the package it came in). Subtract your child’s measurement from the total tube length, and write it down, too. We will call this the “extra tube length” number. Keep it handy; you will use it later to make sure the tube is placed properly. Extra tube length:
- Now, from the tip of the tube, measure the distance of your child’s measurement (in the pictured example this would be 12 inches). Mark that spot on the tube using a permanent marker. Now you are ready to insert the feeding tube.
Insert the tube:
- Wash your hands.
- Gather equipment:
- feeding tube
- formula
- gauze if needed
- water for lubrication or other lubricant
- pH testing strips
- syringe, size:
- tape, type:
- water for rinsing if needed
- Position the child.
___ Swaddle an infant (wrap with the arms secured in a blanket). Put the infant on the left side, either in an infant seat or on a bed, with the head raised.
___ Older children should be placed in a comfortable position, and may be held by an adult if they wish. Some children may vomit when the tube is put in. Be sure the child can be turned easily if this happens. Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay. - Lubricate the tube with water or put a small amount of lubricant on the end of the tube if you have been taught to do so. Most tubes have a coating that is activated with water, making the tube easier to slide in.
- Insert the tube into the nostril, pushing the tube gently down until the mark on the tube is at the tip of the nose. Older children can drink or swallow to help the tube go down. Infants may suck on a pacifier or your fingers during tube insertion. This can be uncomfortable for your child and it is normal for the child to cough or sneeze while the tube is being inserted. It may be best to have someone help you.
After the tube is inserted, remove the tube right away if:
- coughing
- gagging
- sneezing
- vomiting
- wheezing
- changing color
- cannot catch a breath
- change in respiratory rate
- change in oxygen needs
- decrease in pulse oximeter readings
- increased restlessness
- unexplained irritability, discomfort, or abdominal pain
- cannot talk or change in the quality of cry
- or you see the tube coming out of the mouth
- Cuddle and comfort your child for a few minutes, and try again.
- Once the tube is in place, secure it with tape as shown by the nurse.
- Check the tube placement (see below).
Checking the tube placement
To prevent aspiration, you must check the tube placement before each feeding, to be sure it has not moved. The stomach should be as empty as possible when checking for placement, so time each placement check before medications or feedings.
- Look at your child. Is your child comfortable and breathing normally? If the child appears distressed, gagging, sneezing, vomiting, wheezing, changing color, cannot catch a breath, change in respiratory rate, change in oxygen needs, decrease in pulse oximeter readings, increased restlessness, unexplained irritability, discomfort, or abdominal pain, cannot talk or change in the quality of cry, or you see the tube comming out of the mouth: Do not start the feeding.
- Make sure that the mark on the tube is at the nostril. Measure the tube from the mark at the nostril to the beginning of the hub and make sure it matches the “extra tube length” number you wrote down earlier. (See “Get ready,” step 7, above.) If you cannot see the mark or the length has changed, do not start the feeding. Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay.
- Check placement with a pH strip. Try to pull out some stomach fluids with the syringe. Using a small syringe (3 to 5 ml) will make this easier. Test the acidity of the stomach fluids with a pH strip. A pH of less than 6 indicates proper placement. A pH of 6 or higher may indicate incorrect placement. If you get a pH of 6 or greater, call your doctor. Note: With a 3.5 or smaller “neotube” you may not be able to pull out stomach fluids.
- Baseline pH .
- If unable to obtain pH but length, measurement and child’s condition are unchanged, may start the feeding.
Paying careful attention to these signs will help you to be sure that the tube is placed correctly. If you have any doubts, it is best to remove the tube and replace it.
Giving the feedings
___ Bolus feeding
It may be helpful to have 2 people to do this type of tube feeding. One person can hold and comfort the child while the other gives the feeding.
- Wash your hands.
- Measure the correct amount of formula and warm it to the desired temperature.
- Check tube placement as above (observing mark on NG tube and pH testing).
- Clamp the tube.
- Attach a syringe to the feeding tube.
- Pour the formula into the syringe.
- Unclamp the tube.
- Allow the formula to run for the same amount of time as it would take the child to drink it by mouth, or as prescribed by the doctor.
- Ways to help the feeding flow:
Try to start the feeding when the child is calm. You may have to “push” the feeding to get it started. To do this, place a plunger into the syringe and push slightly. Remove the plunger gently and allow the formula to flow in by gravity. If your child is crying, you may need to repeat the push several times.ORDER A PLAGIARISM-FREE PAPER NOW
___ A pacifier may help calm a young child and also helps to connect sucking with stomach-filling.
___ For older children, use activities to distract them, or involve the child with the feeding, such as holding the syringe. - During the feeding, keep the bottom of the syringe no higher than 6 inches above the child’s stomach.
- Continue adding formula into the syringe until the prescribed amount is given.
- When the syringe is empty, flush the tube with the prescribed amount of warm water.
- After the feeding:
___ Clamp the tube.
___ Leave the tube open to air. Tape a piece of gauze over the syringe to keep fluids from splashing out.
___ Burp your child.
___ Infants and young children may be most comfortable with their head and upper body raised, or lying on their left side.
___ Older children may be up and playing.
___ Continuous feeding with a feeding pump
- Wash your hands.
- Measure enough formula for 4 hours and warm it if needed.
- Pour formula into the feeding bag. Run formula to the end of the pump tubing.
- Set up the pump and pump tubing according to the directions from the medical supply company. Be sure the rate is set correctly.
- If a new feeding tube is to be inserted, see “Getting ready to insert the tube” and “Inserting the tube.”
- Check placement if external tube length measurement is unchanged, exit site mark is visible and there are no changes in your child’s condition, continue feedings without interruption (see “Checking the tube placement”). Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay. If vomiting or respiratory distress occurs at any time, tube placement should be verified.
- Connect the pump tubing to the child’s feeding tube.
- Turn on the pump. Check to make sure the formula is dripping.
- As the bag empties every 4 hours, add more formula.
- Hold and/or talk to your child often during waking hours. Have your child’s head raised during the entire feeding.
- Watch your child carefully to make sure there is no change in breathing or behavior. Make sure the mark on the tube is still at the nostril. It is also a good idea to measure it every few hours, because sometimes the tube can slip under the tape. Stop the feeding if the mark changes and recheck placement.
- If your doctor tells you to, after the feeding period, flush the tube with the prescribed amount of warm water.
- If you are told to stop the continuous feeding:
___ Plug or clamp the tube.
___ Leave the tube open to air. Tape a piece of gauze over the syringe to keep fluids from splashing out.
___ Burp your child.
___ Have child’s head raised for about 30 minutes after the feeding is done.
___ Removing the feeding tube (if ordered)
- Remove the tape.
- Pinch the tubing and pull the tube out in one quick motion.
- Hold, cuddle, and comfort your child. If your child is an infant, burp him or her.
Skin care
Clean your child’s skin around the tube often with warm water, removing any secretions. If the nostril is reddened or the skin is irritated, remove the tube and replace it in the other nostril, if possible.
If you have used a transparent dressing on your child’s face, remove it by loosening it with mineral oil and gently working the dressing off. If you use adhesive remover to loosen the dressing, be sure to wash the skin with water to remove all residue, as this can be very irritating . Nasogastric Tube Insertion for Eternal Feeding in Babies and Infants Essay.
